
Grit. Intention. One step at a time.
“Nature does not hurry, yet everything is accomplished.” — Lao Tzu
This is the technical backbone of my story. Here, I document the surgical architecture behind my amputation — the AMI, TMR, and RPNI work that transformed my right arm from a source of pain into a living interface for future prosthetic systems.
This space is for clinicians, engineers, and the deeply curious —
A place to explore how biology, design, and possibility intersect — and what becomes possible when the body is treated as architecture, not limitation.
From architecture to artistry, a patient perspective
The Choice
For many years, my right arm was defined more by pain than by function. In searching for a better quality of life, I began exploring emerging approaches to complex upper‑limb amputation and reconstruction. Along the way, I found a clinical study using advanced surgical techniques designed to preserve neural signaling and prepare patients for future bionic integration.
I was evaluated, and I was fortunate to be accepted as a strong candidate.
In 2022, I chose to undergo a transhumeral amputation as part of that study — not because I was chasing innovation for its own sake, but because it offered the best chance for meaningful function beyond chronic pain.
The Rebuild
The procedure combined several advanced neurosurgical techniques — AMI, TMR, and RPNI — each intended to preserve communication between brain, nerve, and muscle.
What resulted was not a finished device, but a biological foundation: a residual limb structured to support intuitive control, sensory feedback, and adaptability as prosthetic technology continues to evolve.
At the time, I did not think of it as “getting a bionic arm.”
The Recovery
Recovery unfolded alongside additional surgeries on my remaining wrist and the practical realities of life as a new amputee. Progress was slow, nonlinear, and demanded a kind of patience I didn’t yet know I had.
During this period, Northport, Michigan became a place of steadiness. Physical therapy filled the days. Clay entered the quiet spaces between.
The Discovery
Working with clay began as rehabilitation. It became a way to understand my body again.
Hand‑building demands subtle pressure, timing, and attention — feedback that doesn’t rely on speed or strength. Over time, I realized my reconstruction didn’t limit this work; it shaped how I approached it.
Each piece I make now reflects an ongoing calibration between mind, body, and material — a reminder that function isn’t only mechanical.
The Blueprint
A Biological Interface for Future Systems
The surgical approach used in my reconstruction was not designed around a single prosthetic device. It was designed to preserve and structure biological signals in a way that future technologies — many of which do not yet exist — could reliably access.
What exists today is a human interface.
Proprioceptive Architecture (AMI)
Agonist–Antagonist Myoneural Interfaces (AMI) were created by pairing muscles in functional opposition, mirroring the way muscles naturally work in an intact limb.
Capability:
This architecture allows my brain to receive real‑time information about limb position and movement intent, even without a physical hand attached. The result is natural proprioceptive feedback — a sense of “where the limb is” — rather than relying only on vision or mental guesswork.
Why it matters beyond amputation:
Reliable proprioception is foundational for any system that aims to integrate with the nervous system, including neurorehabilitation, exoskeletons, and closed‑loop human–machine control.
Neural Command Routing (TMR)
Targeted Muscle Reinnervation (TMR) rerouted five major nerves that once controlled my hand into remaining upper‑arm muscles.
Capability:
Distinct movement intentions (such as wrist rotation or hand closure) now produce isolated, measurable muscle signals. These signals are biologically intuitive — they originate from natural motor intent, not from learned substitutions.
Why it matters beyond amputation:
TMR shows that complex neural intent can be reassigned and preserved even after major anatomical change. This has implications for prosthetics, neural decoding, adaptive robotics, and motor‑control research.
Signal Amplification and Stability (RPNI)
Regenerative Peripheral Nerve Interfaces (RPNI) were created by embedding nerve endings into small grafts of my own muscle tissue.
Capability:
RPNIs serve two critical functions:
• Preventing neuromas and chronic nerve pain
• Amplifying neural signals while reducing biological “noise”
This creates cleaner, more stable data streams suitable for long‑term sensor integration.
Why it matters beyond amputation:
Signal clarity and stability are some of the biggest challenges in neural interfaces. RPNI offers a biological solution that grows and adapts with the body rather than fighting it.
What This Enables
Together, AMI, TMR, and RPNI form a biological signal ecosystem capable of:
• Intuitive motor‑intent decoding
• Real‑time proprioceptive feedback
• Long‑term adaptability as technology evolves
This system does not require constant cognitive effort to operate. It aligns with how the nervous system already works.
Why This Isn’t Finished
No external device has yet fully matched the capabilities of the biological interface that now exists inside my arm. That gap — between what the body can provide and what technology can currently receive — is where future work lives.
Until then, this blueprint remains active, responsive, and quietly waiting.
Five Years Inside the Upper-Limb System
Over the past five years, I have immersed myself in understanding the realities of upper-limb prosthetics — not only as a patient, but as a daily user working in physically demanding environments and the challenges of overload to the complication of my remaining wrist, preserve my independence.
This experience includes navigating:
• Insurance approval pathways
• Socket design and fabrication techniques
• Market component limitations
• Biomechanical leverage challenges
• Gender-specific fitting considerations
• Functional abandonment patterns
Patient-Led Socket Development
After multiple conventional fittings failed to provide distal stability and usable leverage, I began testing modifications.
Core observation:
Traditional transhumeral sockets often prioritize proximal suspension without sufficiently stabilizing the distal limb under load. When extended components are attached, this can create rotational instability and inconsistent pressure distribution.
My approach included:
• Requesting casting on a Magliner
• Prioritizing distal-end stabilization over suction pull
• Building up the narrowed distal fabrication area manually, prototype to fabrication added a void from current laminating ring process.
• Adding rubber ring compression for increased contact security
• Adhering a neodymium magnet at the base to provide strong stabilization with Magliner. Available Maglock systems proved bulky and required excessive release force. Streamlined attachment became essential.
To avoid a harness system — particularly restrictive for female anatomy — I designed a BOA-adjusted socket that allowed controlled compression. Many previous sockets restricted that movement. This one did not.
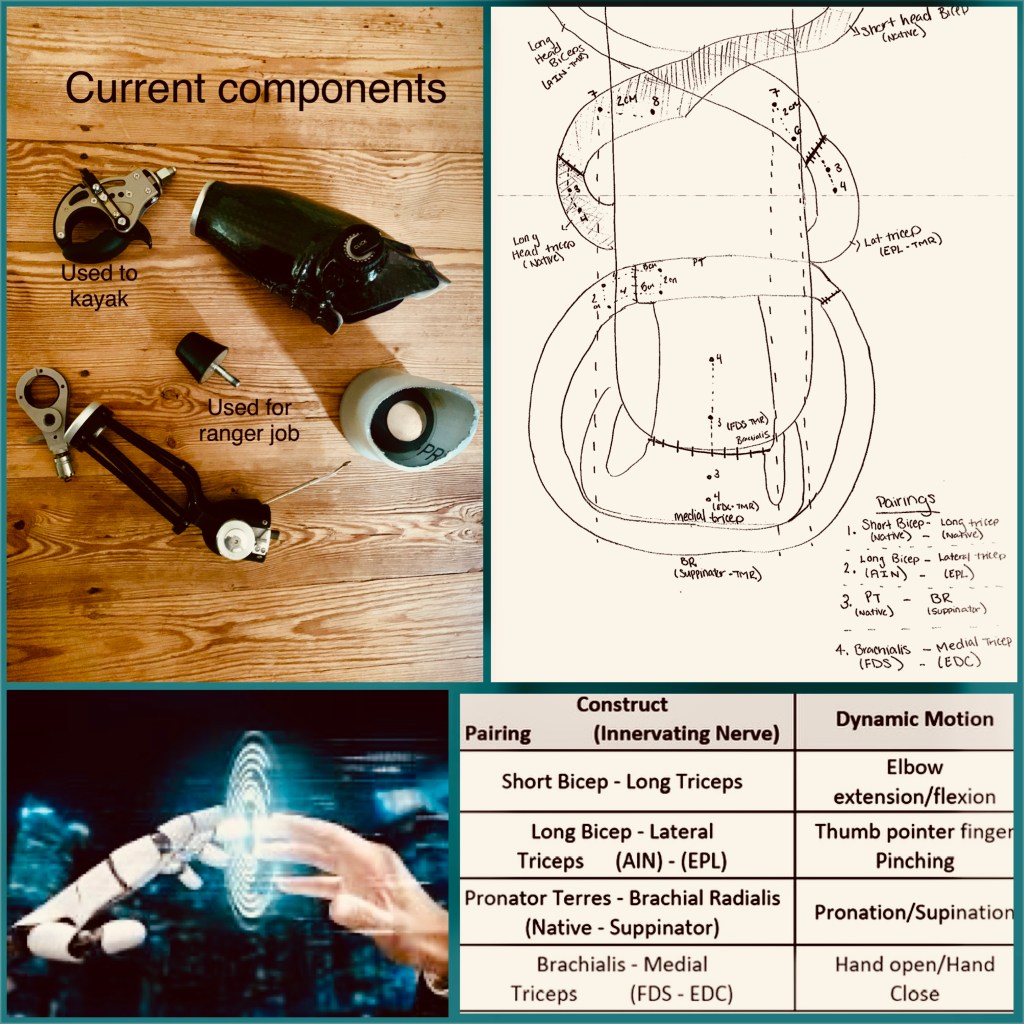
Mechanical Adaptation in the Field
When standard elbow components proved incompatible — including thread systems largely unchanged since mid-century Hosmer designs — I fabricated a double-thread conversion adapter.
This allowed attachment of:
• A 1964 Mustang hood bumper (lightweight, shock-tolerant, durable)
• A Jaw II terminal device for kayak anchoring
• Configurations functional for shoveling, sweeping, and ranger duties
The gap created by the thread adapter unexpectedly improved leverage.
This was not aesthetic. It was functional survival.
Myoelectric Attempt — System Friction
After complications in my remaining wrist, I re-entered the myoelectric pathway.
Insurance approval, a daunting one year.
The approval window allowed less than two months for fabrication and delivery.
The device remains in limbo.
Current barriers include:
• Outdated socket paradigms
• Heavy component architecture
• Battery bulk and placement
• Difficulty engaging AMIs, TMRs, and RPNIs within conventional layouts
• Limited incremental testing models
My current strategy:
Begin with a stabilized socket similar to my current, with adjustments for direct electrode placement with a BOA system.
Snap electrodes using the Magliner.
Integrated battery on-board on socket.
An advanced elbow with short forearm.
Two-fold objective:
- Activate and strengthen native AMI constructs while developing intuitive elbow control.
- Reduce system bulk before extending to a full distal hand.
Build the elbow before the hand.
Strengthen the shoulder before extending load.
On Osseointegration — Consideration, Not Rejection
I have been approached as a candidate for E-OPRA osseointegration.
I do not dismiss its promise.
However, I believe there may be architectural pathways worth exhausting before introducing long-term skeletal interface risk with the current complications.
I remain open — and cautious.
The question is not whether osseointegration works.
The question is whether we are fully exploring less invasive interface solutions.
The Larger Pattern
Upper-limb prosthetics operate within a constrained ecosystem:
• Small market size
• High development cost
• Fragmented manufacturing pipelines
• Insurance definitions of “medical necessity” that prioritize presence over usability
The limitation is not intelligence or effort.
It is translation — from laboratory capability to daily function.
My Vision
I envision:
• Lightweight distal stabilization systems
• Electrode mapping aligned directly with AMI architecture
• Modular elbow-first development pathways
• Streamlined integrated power systems
• Patient-driven testing models
My limb is biologically prepared for closed-loop control.
The external system is still catching up.
Collaboration
What I offer is not complaint.
It is longitudinal field data.
Five years of lived biomechanics.
Socket failure analysis.
Interface experimentation.
Daily-use testing under load.
This is ongoing documentation. Not a conclusion.
Field Notes:
This section is my ongoing log — small observations, adjustments, and questions as function continues to develop, tracking of what I feel and what works.
